
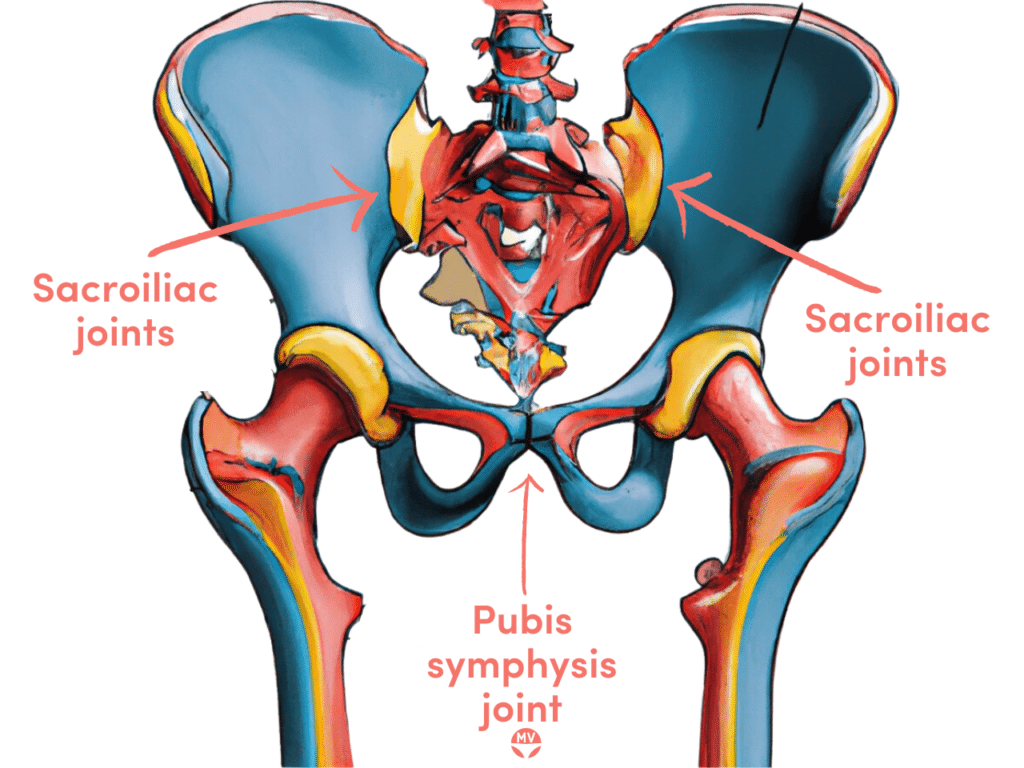
Osteitis pubis is a chronic, non-infectious inflammation and pain of the pubic symphysis – the joint at the front of the pelvis where the two pubic bones meet1.
It’s typically set off by repetitive stress across that joint, known as ‘shearing’, which comes from surgery, accidents, having one leg longer than the other, or biomechanical foot or shoe issues.
Muscle problems, inflexibility, sacroiliac (SI) joint dysfunction or joint misalignment can create unusual shearing forces that trigger and aggravate tiny injuries (microtrauma), leading to inflammation, pain and muscle spasms.
Causes of osteitis pubis
Pregnancy can be a major contributing factor, alongside pelvic surgery or major physical trauma. Repeated minor trauma – especially from sport – is a common driver, and sometimes there’s a rheumatological cause behind it1.
It’s particularly common in athletes whose sports involve kicking, sprinting, and sudden changes of direction, where the joint is loaded again and again through single-leg stance2.
Everyday contributing factors include running on concrete, going from zero to hero with a new exercise routine, wearing poorly fitting shoes, movement disturbances and stiff muscles. Everyone’s biomechanics and body are different, though, so it’s best assessed individually by an experienced professional.
Symptoms of osteitis pubis
- Lower pelvic pain and aching – groin, hip, bladder, clitoris, vagina, perineum, scrotum or testicles
- Painful sex (dyspareunia)
- Pain that’s worse with coughing, sneezing, sitting, standing, lying on one side, changing direction, kicking, pivoting on one leg, running or jumping
- Clicking or popping when walking or during vigorous movement
- Loss of flexibility through the groin
- Pain that may be a dull ache, a sharp stab, or tenderness to the touch
- In pregnancy, relaxin loosens the pelvic ligaments, which can let the joint shift and become painful – known as symphysis pubis dysfunction (SPD)3
- May worsen after birth or pelvic surgery
- May contribute to pelvic floor muscle dysfunction
Because that pain can land in the clitoris, vagina, perineum or show up as painful sex, osteitis pubis is easy to mistake for a gynaecological problem – so it’s worth having the pelvis properly assessed rather than assuming the cause.
Diagnosing osteitis pubis
On a healthcare practitioner’s recommendation, an X-ray, CT or other scan can visualise and confirm osteitis pubis. Irregularity and widening of the pubic symphysis are the key findings2.
Spinal, pelvic and lower-limb biomechanics should also be assessed to look for misalignments and muscle or ligament tension or laxity. The main things to tell it apart from are pubic symphysis dysfunction (SPD), a hernia, or a groin strain.
Treating osteitis pubis
Most cases settle with conservative, hands-on care rather than surgery, so this is really the territory of a physiotherapist or sports-medicine practitioner. We don’t do manual or physical treatment ourselves at My Vagina, so that side is best handled by one of them.
Treatment usually centres on realigning and mobilising the sacroiliac and pubic symphysis joints, settling the inflammation and pain, and then rebuilding stability with strengthening and movement re-education. A pelvic support belt can help, and anti-inflammatory measures, stretching and strengthening all play a part1.
There’s no single standard treatment, and newer approaches are still being developed. Surgery is a last resort for severe cases only – the success rate is low, and further problems from the surgery itself are not uncommon.
The pubic symphysis joint is also called the pubis symphysis, symphysis pubis or symphysis pubica.
Frequently asked questions
Is osteitis pubis serious?
It’s not dangerous, but it can be painful and slow to settle, and it can really interfere with movement, exercise and sex while it’s active. Most people recover well with conservative treatment and time.
How long does osteitis pubis take to heal?
It varies a lot, and recovery is often measured in months rather than weeks, especially if the underlying biomechanics aren’t addressed. Rushing back to full activity too soon tends to set it off again.
Can osteitis pubis cause vulval pain or painful sex?
Yes. The pain can radiate into the clitoris, vagina, perineum or groin and can make sex painful, which is why it’s sometimes mistaken for a gynaecological issue. If pelvic pain isn’t adding up, the pubic symphysis is worth checking.
This article is general information and not a substitute for personalised medical advice. If you have ongoing pelvic or groin pain, please see an experienced practitioner.
References
- Dirkx M, Vitale C. Osteitis pubis. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
- Beatty T. Osteitis pubis in athletes. Current Sports Medicine Reports. 2012;11(2):96-98.
- Aldabe D, Ribeiro DC, Milosavljevic S, Bussey MD. Pregnancy-related pelvic girdle pain and its relationship with relaxin levels during pregnancy: a systematic review. European Spine Journal. 2012;21(9):1769-1776.


