
Hyperreactio luteinalis is a benign, pregnancy-related swelling of both ovaries, caused by multiple fluid-filled cysts. It is driven by the pregnancy hormone human chorionic gonadotrophin (hCG), it almost always settles on its own after birth, and despite looking alarming on a scan it is not cancer.1–2
Trouble is, grossly enlarged, multicystic ovaries in pregnancy can be mistaken for an ovarian tumour, and that fear has historically led to unnecessary surgery – sometimes the removal of perfectly healthy ovaries.1–2
Recognising the condition for what it is matters, because most cases just need careful monitoring rather than surgery.
We meet women and pregnant people who have been frightened by an incidental scan finding. And our job is to work with their medical team to understand the problem and support where it helps. As experienced vulvovaginal specialist naturopaths, there is rarely a time we can’t help in some way – whether that’s supporting their management, easing discomfort, or helping recovery along.
What is hyperreactio luteinalis?
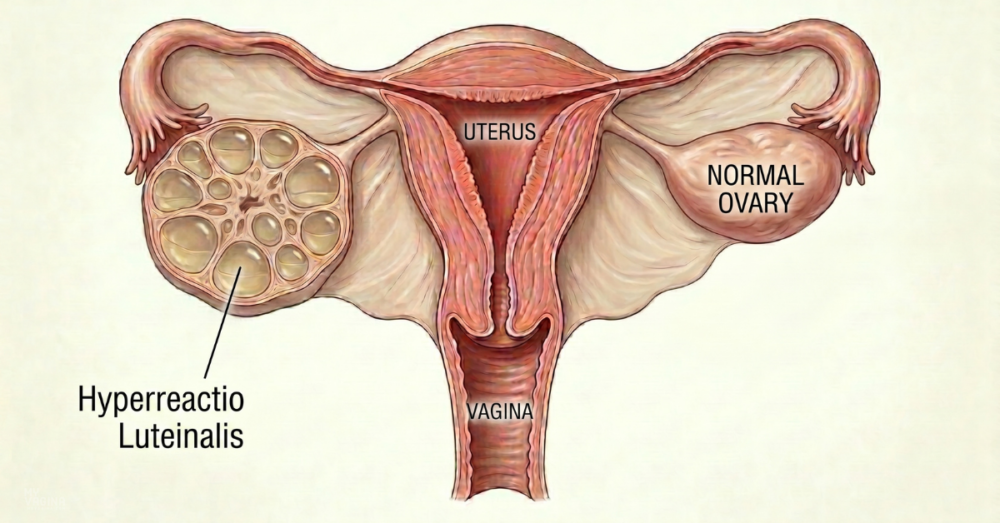
Hyperreactio luteinalis is a condition in which the ovaries enlarge during pregnancy because they fill with many benign theca-lutein cysts.1 It is the most dramatic end of a spectrum of functional ovarian cysts seen in pregnancy. And it is uncommon – the medical literature is built almost entirely from individual case reports rather than large studies.1–2
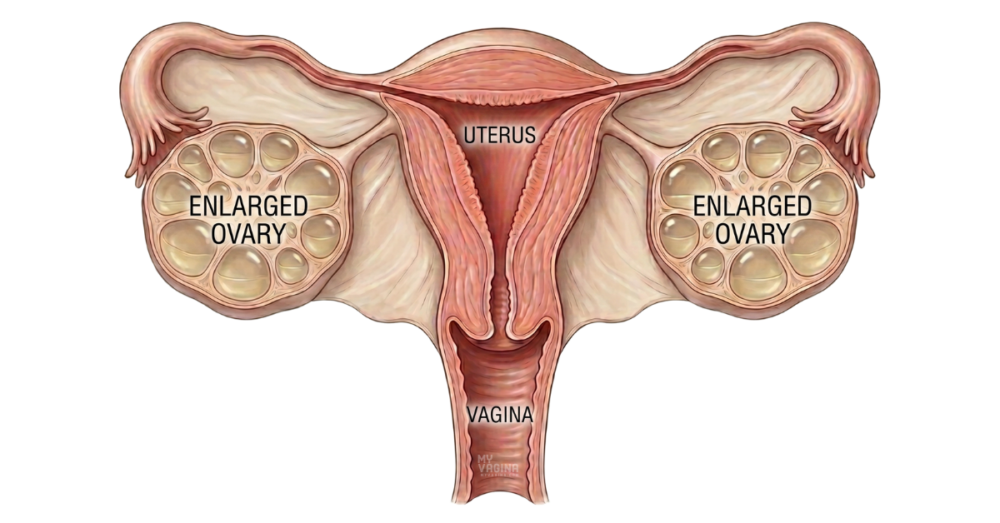
The cysts are thin-walled and usually affect both ovaries, although rare one-sided cases exist.1 The enlargement can be pronounced. Ovaries that would normally be a few centimetres across (an inch or two) can reach an average diameter of around 15 cm (about 6 inches, roughly the size of a grapefruit), occasionally swelling to a volume of about 1.5 litres (around 1.6 US quarts, about the size of a large soft-drink bottle).1–2
It is one of three functional cyst types that turn up in pregnancy, alongside follicular cysts and corpus luteum cysts, and it is the least common of the three.2 You can read more about the wider group in our guide to ovarian cysts.
What causes hyperreactio luteinalis?
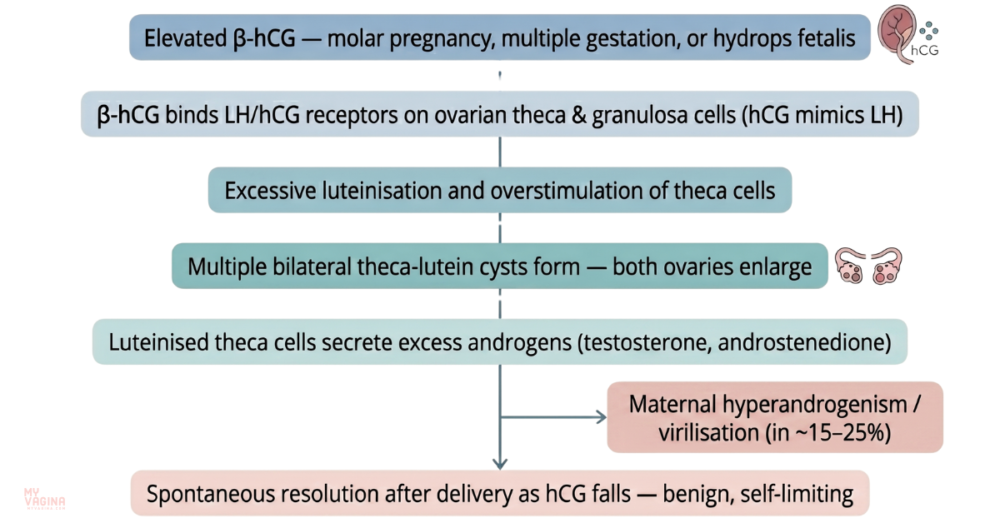
The ovaries respond to hCG, the hormone that rises steeply in early pregnancy. In hyperreactio luteinalis, the ovaries overreact to this signal – either because hCG levels are abnormally high, or because the ovaries are unusually sensitive to normal levels.1–2 The result is exaggerated cyst formation, and in some people a surge in androgen (male-type hormone) production from the stimulated ovarian tissue.3
This is why it tends to show up when the body is making a lot of the pregnancy hormone hCG, or the placenta is unusually large. That includes a molar pregnancy and related conditions, where placental tissue overgrows instead of forming a normal pregnancy (gestational trophoblastic disease, including the rare cancer choriocarcinoma); carrying twins or more; rhesus sensitisation, where the mother’s immune system attacks the baby’s blood cells and the baby can become very swollen with fluid (hydrops); diabetes in pregnancy; and fertility medicines used to trigger ovulation.2
Importantly, it also happens in completely ordinary single pregnancies with normal hCG, where ovarian hypersensitivity rather than excess hormone seems to be the driver.1–2
The thyroid connection
There is a less obvious driver worth knowing about. In untreated underactive thyroid (hypothyroidism), very high levels of thyroid-stimulating hormone (TSH) can cross-react with the ovarian receptors that normally respond to hCG and follicle-stimulating hormone, over-stimulating the ovaries.4 In at least one reported case, simply correcting the thyroid with levothyroxine shrank the ovaries and settled the raised androgen levels.4
It is the kind of root cause we always want to rule out. In our experience here at My Vagina, an unrecognised thyroid or hormonal issue can present with dramatic symptoms, and we’re always keeping an eye out for what lies beneath them.
Not the same as ovarian hyperstimulation
Hyperreactio luteinalis is sometimes confused with ovarian hyperstimulation syndrome, which produces similar-looking enlarged, multicystic ovaries.2 The key difference is the trigger: ovarian hyperstimulation syndrome typically follows fertility treatment with ovulation-induction drugs, whereas hyperreactio luteinalis is a response to the pregnancy itself.2
Is hyperreactio luteinalis dangerous?
For most people it is not. The condition tends to be self-limiting, with the ovaries returning to normal on their own after delivery and no lasting harm to mother or baby.1 The main risks come from the sheer size of the ovaries and from the hormonal changes, not from the cysts being malignant.1–2
Possible complications include twisting of an enlarged ovary (torsion), cyst rupture, bleeding, a build-up of fluid in the abdomen, and pressure-related discomfort or breathlessness.2–3 There is also a recognised association with high-hCG pregnancy complications such as pre-eclampsia, so the small subset of people with very abnormal hCG levels may warrant closer monitoring.1
What it feels like
Many cases cause no symptoms at all and are picked up by chance, either on a routine third-trimester ultrasound or during a caesarean.1 When there are symptoms, they may include abdominal swelling or discomfort, sudden severe pain if a cyst twists or ruptures, or signs of raised androgens.2
Virilisation in the mother
Raised androgen levels produce signs of virilisation – acne, oily skin, excess hair growth (hirsutism) and, less often, a deepening voice. These signs appear in up to about a third of people with the condition.1,3 They are usually temporary: androgen levels fall after birth and the changes typically reverse, although the voice can be slower to recover.3
What about the baby?
Reassuringly, virilisation of a female foetus (enlarged clitoris and other signs) is rare, even when the mother shows clear signs.1,5 The placenta carries an enzyme called aromatase that converts much of the excess testosterone into oestrogen before it reaches the baby. This protects the foetus in a way that does not happen with some androgen-producing ovarian tumours.5 Where it does occur, it depends on the timing and severity of the hormone surge.1
How is it diagnosed?
Ultrasound is the workhorse. Enlarged ovaries packed with multiple cysts often show a characteristic ‘spoke-wheel’ pattern, with normal blood flow on Doppler imaging, which helps distinguish the condition from a tumour.1,4 On a scan report this is often written up as multicystic ovaries, or cysts on both ovaries. You can read more about this kind of scan in our guide to the transvaginal ultrasound.
Because the ovaries can look so abnormal, the most important step is to consciously consider hyperreactio luteinalis and avoid jumping to a cancer diagnosis.1 Where there is genuine doubt at the time of surgery, a small biopsy and a frozen-section examination can confirm the benign nature of the tissue before any ovary is removed.2
Blood tests may show raised androgens, but testosterone levels do not reliably predict who will show outward signs of virilisation.1
How is hyperreactio luteinalis treated medically?
For uncomplicated cases, the mainstay of treatment is conservative management – essentially careful watching with reassurance, because the cysts resolve on their own after delivery.2–3 The strongest message from the medical literature is to resist the urge to operate, since unnecessary surgery risks the ovaries and future fertility.1–2
Surgery is reserved for specific problems rather than the cysts themselves. It is needed mainly to deal with a twisted ovary, a ruptured cyst, or significant bleeding, and even then the aim is to conserve as much ovarian tissue as possible.2–3
Where an underlying driver can be identified and treated, it should be. Correcting unrecognised hypothyroidism with thyroid hormone replacement is one clear example, and it can resolve both the ovarian enlargement and the raised androgens.4
Birth and feeding
Vaginal birth is generally preferred where obstetrically appropriate, and the condition itself does not dictate a caesarean.1 One practical detail is breastfeeding: high androgen levels can interfere with milk production, so support to establish and sustain feeding while those hormone levels fall after birth is worth planning for.1
Recovery and recurrence
The ovaries usually shrink back to normal within about 6 to 12 weeks of giving birth, though resolution is occasionally slower and a small number of cases have taken many months.3 There is some evidence of a genetic predisposition, and the condition can recur in a later pregnancy, so a history of hyperreactio luteinalis is useful information for future antenatal care.1
Functional and integrative medicine approaches to hyperreactio luteinalis
There is no special herbal or supplement ‘protocol’ that treats hyperreactio luteinalis, and it would be wrong to suggest otherwise. This is a pregnancy condition that belongs in the care of an obstetric team. A sensible integrative approach works alongside that care, not instead of it.
Functional thinking comes into its own in the root-cause questions. The medical literature already points to drivers worth investigating: thyroid function, because untreated hypothyroidism can stimulate the ovaries,4 and a pre-existing tendency to hyperandrogenism, since conditions linked to higher androgens may make the ovaries more reactive.3 Checking thyroid status properly, and understanding someone’s hormonal background, is squarely within an integrative clinic’s scope.
The rest is about support. Reassurance does a lot of work here, because the gap between how frightening the scan looks and how benign the condition usually turns out to be can be enormous. Practical help with the temporary skin and hair changes, and planning ahead for breastfeeding while androgens settle, both matter too.
In our experience, the most useful thing we do for someone with an alarming scan finding in pregnancy is help them actually understand it, check whether anything safely treatable is sitting underneath, and steer them away from surgery they do not need.
What patients should not do is self-treatment, attempt to ‘shrink’ the cysts with supplements, or delay obstetric review. Any sudden severe abdominal pain, in particular, needs urgent medical assessment to rule out torsion or rupture.2–3
Frequently asked questions
Is hyperreactio luteinalis a cancer?
No. It is a benign condition, but because the swollen, multicystic ovaries can look like a tumour on imaging it is sometimes mistaken for one, which is exactly why awareness of it matters.1–2
Will it go away after the baby is born?
Almost always. The ovaries usually return to normal within about 6 to 12 weeks of delivery, occasionally taking longer.3
Does it harm the baby?
Generally no. Virilisation of a female foetus is rare because the placenta converts much of the excess androgen into oestrogen before it reaches the baby.1,5
Why are my ovaries producing male hormones?
The same hCG over-stimulation that creates the cysts can prompt the ovarian tissue to make extra androgens. This is what produces signs such as acne or extra hair growth in up to about a third of cases.1,3
Can pregnancy cause facial hair, acne or a deeper voice?
It can, in this condition. When the over-stimulated ovaries make extra androgens, some people develop acne, oily skin, extra facial or body hair and, less often, a deeper voice. These signs of virilisation appear in up to about a third of cases and usually fade after birth as hormone levels fall, though the voice can be slower to recover.1,3
Do I need surgery?
Usually not. Uncomplicated cases are watched rather than operated on. Surgery is reserved for complications such as torsion, rupture or bleeding, and even then surgeons try to preserve the ovary.2–3
Can it happen again in another pregnancy?
It can. Recurrence has been reported, and there may be a genetic predisposition, so it is worth mentioning to whoever cares for you in a future pregnancy.1
Is it the same as ovarian hyperstimulation syndrome?
No. The ovaries can look similar, but ovarian hyperstimulation syndrome usually follows fertility treatment, whereas hyperreactio luteinalis is a response to the pregnancy itself.2
Could my thyroid be involved?
Possibly. An untreated underactive thyroid can over-stimulate the ovaries, and in reported cases correcting the thyroid resolved the problem, so thyroid testing is reasonable.4
What to do next
If you have been told you have enlarged or multicystic ovaries in pregnancy, the most important step is to stay under the care of your obstetrician or maternity team. They can monitor the ovaries and check for any underlying driver such as thyroid or hormonal issues. Seek urgent care for any sudden, severe abdominal pain.
If you would like to talk through what a result means, or which root-cause questions are worth raising with your team, you can ask Aunt Vadge’s Assistant using the chat widget in the bottom left of the screen. Or book time with one of our practitioners for a more thorough look at the hormonal picture.
This is general information, not a substitute for personalised medical advice. If you have symptoms or concerns, please see your healthcare provider.
- Malinowski AK, Sen J, Sermer M. Hyperreactio Luteinalis: Maternal and Fetal Effects. J Obstet Gynaecol Can. 2015;37(8):715–723.
- Kurakula S, Muralidharan V, Appaneravanda LC, Navya N, Gayathri KB. Rupture of Bilateral Theca Lutein Cysts During Pregnancy: A Case Report. Cureus. 2022;14(9):e29758.
- Kim S, Lee I, Park E, et al. Delayed postpartum regression of theca lutein cysts with maternal virilization: A case report. Clin Exp Reprod Med. 2021;48(4):380–384.
- Chauhan YV, Dalwadi PP, Gada JV, Varthakavi PK, Bhagwat N. Unrecognized Primary Hypothyroidism As a Possible Cause of Hyperreactio Luteinalis. Cureus. 2021;13(2):e13573.
- Baxi LV, Grossman LC, Abellar R. Hyperreactio luteinalis in pregnancy and hyperandrogenism: a case report. J Reprod Med. 2014;59(9–10):509–511.


