
Vulvar pyoderma gangrenosum is a rare, painful, rapidly enlarging skin ulcer on the vulva that is driven by the immune system, not by an infection.1 Despite the frightening name, there is no true gangrene and nothing is ‘eating’ the tissue. It is known as a neutrophilic dermatosis, which means the body’s own first-responder immune cells (neutrophils) flood the skin and break it down.2
Because it looks like an infected sore, it is very often mistaken for herpes, a sexually transmitted infection, a Bartholin’s abscess or an ordinary wound infection. That matters, because the usual response to those problems – cutting, draining, debriding – tends to make pyoderma gangrenosum dramatically worse.3
It is uncommon anywhere on the body, and rarer still on the vulva, but when it does appear, it is frequently misdiagnosed and mistreated for a long time before anyone correctly identifies it. This is a condition for a doctor, ideally a dermatologist working alongside your other specialists, and not something to manage at home.
What is vulvar pyoderma gangrenosum?
Pyoderma gangrenosum (PG) is an inflammatory, non-infectious ulcer that belongs to a family of conditions called the neutrophilic dermatoses.1
In genetically susceptible people, both the innate and the adaptive immune system become dysregulated, the inflammasome over-fires. And a neutrophil-dominant flood of inflammatory messengers (tumour necrosis factor-alpha, interleukin-1, interleukin-17, interleukin-23 and others) tips the skin into ulceration.2
There are four classic forms: ulcerative (the most common), pustular, bullous and vegetative. Vulvar PG is usually the ulcerative type, appearing on the labia, the perineum or around the perianal skin.1
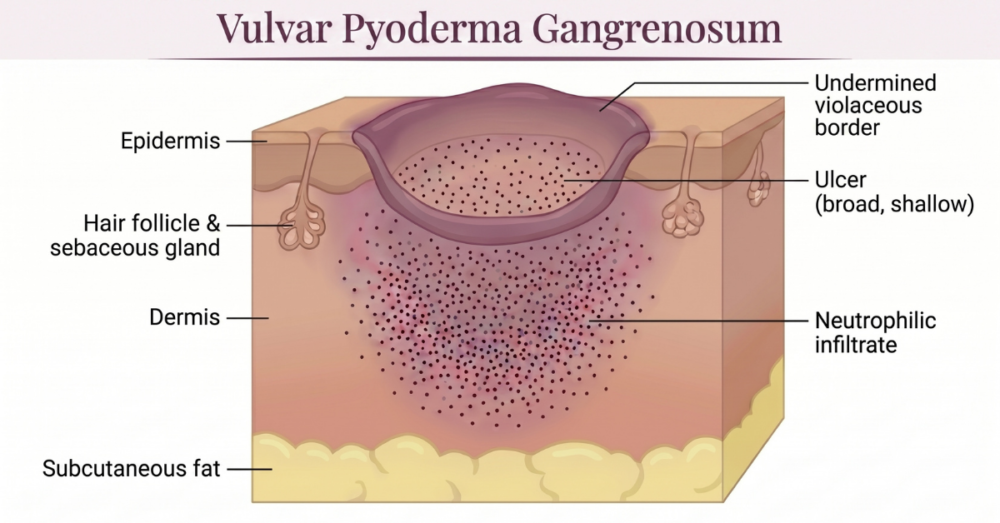
It typically starts as a small tender papule, pustule or what looks like a ‘spider bite’, then breaks down over days into a deepening ulcer with a ragged, overhanging, violet-coloured edge and a ‘boggy’ base.1 The pain is usually out of all proportion to the size of the wound.
What causes it, and why the vulva?
The exact cause is still not fully understood, but PG is best thought of as a sign of a misfiring immune system rather than a local skin problem.2 The skin is where the storm shows up, but the weather system usually sits deeper in the body.
More than half of people with PG have an associated systemic condition. In a meta-analysis of more than 2,600 patients, an underlying disease was present in about 57 per cent of cases, the most common being inflammatory bowel disease (around 18 per cent), inflammatory arthritis (around 13 per cent), blood disorders and cancers of the blood (around 9 per cent) and solid tumours (around 7 per cent).4
On the vulva specifically, links to Crohn’s disease and to blood disorders come up repeatedly in the case literature.3
Genital pyoderma gangrenosum has a pattern of its own. An early 2025 systematic review that pooled 84 reported cases of genital PG – presented so far only as a conference abstract, so the figures are preliminary – found the vulva and penis to be the most commonly affected genital sites, and that most cases were idiopathic, with no underlying disease identified.5
Where a trigger was found it was usually surgical, with episiotomy a recurring factor in women and people with vaginas. And the comorbidities that did appear were led by blood disorders (around 13 per cent) and inflammatory bowel disease (around 12 per cent).5
The second piece of the puzzle is pathergy – the tendency for PG to erupt or spread at sites of skin injury. Around 16 per cent of cases are triggered by trauma to the skin.4 On the vulva, that trauma can be something as routine as an episiotomy, a vaginal tear during birth, a biopsy, shaving or surgery. One reported case described vulvar PG developing in the exact site of a previously healed obstetric laceration.3
This is why PG can be so cruelly self-perpetuating. The wound looks infected, so it gets debrided or incised, the pathergy response kicks in, and the ulcer grows. It is also why a thorough work-up matters more than another round of antibiotics.
How is vulvar pyoderma gangrenosum diagnosed?
For a long time PG was called a ‘diagnosis of exclusion’, meaning everything else had to be ruled out first. That has changed. A validated set of criteria, agreed by an international panel of experts, now allows a positive diagnosis.1
Under these criteria, the one essential (major) requirement is a biopsy taken from the edge of the ulcer that shows evidence of a neutrophilic infiltrate.1
Alongside that, four of eight minor criteria need to be met, including exclusion of infection, a history of pathergy, a history of inflammatory bowel disease or inflammatory arthritis, and a rapid response to immunosuppressive treatment.1
Meeting the major criterion plus four minor ones identifies PG with about 86 per cent sensitivity and 90 per cent specificity.1
In practice, that means swabs and cultures are taken and come back negative for bacteria, fungi and viruses, syphilis is excluded, and a biopsy is done from the ulcer edge.3 A biopsy can itself provoke a little pathergy, but it remains important – partly to confirm the picture and partly to exclude the conditions that really mimic PG.1
Differential diagnoses: what else could it be?
The vulvar mimics worth excluding include genital herpes and other non-sexually-transmissible causes of genital ulcers, Behçet disease, hidradenitis suppurativa and, at the most urgent end, necrotising fasciitis. This is a surgical emergency and the one diagnosis you actually cannot afford to miss in the other direction.
Medical treatment for PG
Treatment has two jobs at once: calm the overactive immune response and protect the wound from further injury. Because PG is uncommon, much of the evidence comes from small studies, but a clearer picture has emerged in the last decade.6
Systemic corticosteroids (such as prednisolone) and ciclosporin are the two best-evidenced first-line systemic treatments.7
A UK randomised controlled trial of 112 patients compared the two head to head and found no meaningful difference between them across healing speed, pain and quality of life. So the choice often comes down to the individual’s other health conditions.7
For vulvar PG in particular, ciclosporin has healed wounds that had been worsening despite ordinary wound care.3
For more stubborn disease, or where there is an associated inflammatory bowel disease, biologic medicines that block specific inflammatory messengers – particularly the tumour necrosis factor-alpha inhibitors – have become close to first-line, with other targeted agents now in use or in trials.6 Topical anti-inflammatory and immune-modulating treatments, gentle wound dressings and proper pain control round out the plan.6
One principle sits above all the others: avoid aggressive surgery and debridement on active disease wherever possible, because of pathergy.3 When surgery really cannot be avoided, it is safest done once the disease is already under control with medication.
The functional and integrative approach
At My Vagina we treat holistically, which here means looking past the ulcer to what is fuelling it. PG is rarely a stand-alone skin event. So the single most useful integrative step is also the most orthodox one: find and properly treat any underlying driver, whether that is inflammatory bowel disease, an inflammatory arthritis or a blood disorder.4 Settle the systemic fire and the skin usually follows.
The gut–skin connection is more than lip service here. Inflammatory bowel disease is the most common condition sitting behind PG, so an anti-inflammatory, gut-supportive way of eating and living is a sensible foundation alongside specialist care.4 This is supportive work, not a cure, and it sits beneath medical treatment rather than replacing it.
Because PG produces a chronic, leaking wound, the body’s demand for the raw materials of repair goes up. Adequate protein, vitamin C, vitamin A and zinc all play defined roles in immune function and collagen building during wound healing, and quietly correcting any deficiency is a reasonable, low-risk part of recovery.
Targeted, mechanism-led systemic support – including considered use of herbal medicines for vulvovaginal and female health – can sit alongside, never instead of, your medical team’s plan.
The other really high-value integrative move is protecting the skin from pathergy. That means no picking, no squeezing, no DIY debriding, careful hair-removal choices, and flagging PG to any surgeon or doctor before a procedure on the area.3
Leaving the wound alone is itself a treatment.
Frequently asked questions
Is vulvar pyoderma gangrenosum contagious?
No. It is not an infection and cannot be passed to a partner through sex or contact. It is an inflammatory reaction within your own skin.2
Could it be mistaken for herpes or an STI?
Yes, and it frequently is. Genital PG is often misread as herpes, a sexually transmitted infection or an abscess, which delays the right treatment.3 Negative swabs on a worsening ulcer are an important clue.
Could a vulvar sore that won’t heal be pyoderma gangrenosum?
It is worth considering. A vulvar sore that keeps growing, keeps coming back, or simply will not heal with ordinary care is exactly the kind of ulcer that should raise the question of PG – particularly when swabs for herpes and other sexually transmitted infections keep coming back negative.3
The next step is a doctor, ideally with a dermatology referral, rather than another round of antibiotics on a wound that is not behaving like an infection.
Why shouldn’t the ulcer be cut, drained or debrided?
Because of pathergy. PG tends to flare and spread at sites of injury, so surgery and debridement on active disease can enlarge the wound rather than help it.3 Surgery is safest only once the disease is controlled with medication.
Does having it mean I have a bowel disease?
Not necessarily, but it raises the question. More than half of people with PG have an associated systemic condition, and inflammatory bowel disease is the most common one, so a proper work-up is part of good care.4
Is pyoderma gangrenosum an autoimmune disease?
Not in the classic sense. It is better described as an autoinflammatory condition – the innate, first-responder arm of the immune system misfires and floods the skin with neutrophils, rather than the body making antibodies against itself.2
It does, though, often travel with autoimmune and inflammatory conditions such as inflammatory bowel disease and inflammatory arthritis, which is part of why a proper work-up matters.4
Will it leave a scar?
It often heals with a thin, wrinkled (cribriform) scar. Getting onto effective treatment early, and avoiding repeated trauma, gives the best cosmetic and functional result.1
Can it be cured?
Many people heal well with treatment, though PG can recur, particularly if an underlying condition is not addressed.7 Ongoing follow-up, and treating the driver rather than only the wound, gives the most durable result.
What to do next
If you have a painful vulvar ulcer that is growing, recurring or simply not healing with ordinary care, see a doctor and ask specifically about a dermatology referral. The earlier PG is named, the sooner the right treatment can start and the less tissue is lost along the way.
If you would like to think through the underlying-driver side of things – the gut, immune and systemic picture – alongside your medical care, you can ask Aunt Vadge’s Assistant (the chat widget in the bottom left of the screen). Or book a consultation with one of our practitioners. It can also help to get to know your own anatomy so you notice changes early; our hands-on guide to your vulva is a good place to start.
This is general information, not a substitute for personalised medical advice. If you have symptoms or concerns, please see your healthcare provider.
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a Delphi consensus of international experts. JAMA Dermatol. 2018;154(4):461–466.
- Flora A, Kozera E, Frew JW. Pyoderma gangrenosum: a systematic review of the molecular characteristics of disease. Exp Dermatol. 2022;31(4):498–515.
- Reed BG, Shippey S, Kremp A, Belin E. Vulvar pyoderma gangrenosum originating from a healed obstetric laceration. Obstet Gynecol. 2013;122(2 Pt 2):452–455.
- Kridin K, Cohen AD, Amber KT. Underlying systemic diseases in pyoderma gangrenosum: a systematic review and meta-analysis. Am J Clin Dermatol. 2018;19(4):479–487.
- Comorbidities and diagnostic challenges in genital pyoderma gangrenosum: a systematic review [conference abstract]. J Am Acad Dermatol. 2025. doi:10.1016/j.jaad.2025.05.602.
- Kaur M, Diaz MJ, Anthony M, et al. Treatments for pyoderma gangrenosum: a systematic review and single-arm meta-analysis of systemic therapies. Int Wound J. 2025;22(8):e70733.
- Ormerod AD, Thomas KS, Craig FE, et al. Comparison of the two most commonly used treatments for pyoderma gangrenosum: results of the STOP GAP randomised controlled trial. BMJ. 2015;350:h2958.


