
People who go through menopause because both ovaries were removed tend to get a harder version of the genitourinary syndrome of menopause (GSM) than women who reach menopause naturally. A new study in the journal Menopause compared the two groups and found that surgical menopause was tied to worse vaginal dryness, more painful sex, more urinary trouble and lower sexual desire.1
GSM is not just dryness. It is a whole-system, multidimensional problem, and the way you arrived at menopause shapes how severe it is.1
At My Vagina, we see this pattern in real life. The person who lost their ovaries in one operation often has a faster, fiercer onset of symptoms than someone whose oestrogen tapered away over years. That has direct implications for the vagina (and bladder and everything else!).
What the study found
Researchers led by Dr Samican Ozmen at Torbali State Hospital in Turkey compared 218 women with surgical menopause against 204 women in natural menopause, and measured their genital, sexual and urinary symptoms.1
The surgical-menopause group reported more frequent urination, more painful urination, and more sexual symptoms such as poor lubrication and reduced desire than the natural-menopause group.1
The authors concluded that GSM extends beyond vaginal dryness and constitutes a multidimensional syndrome involving urinary symptoms and sexual function.1
Why surgical menopause hits harder
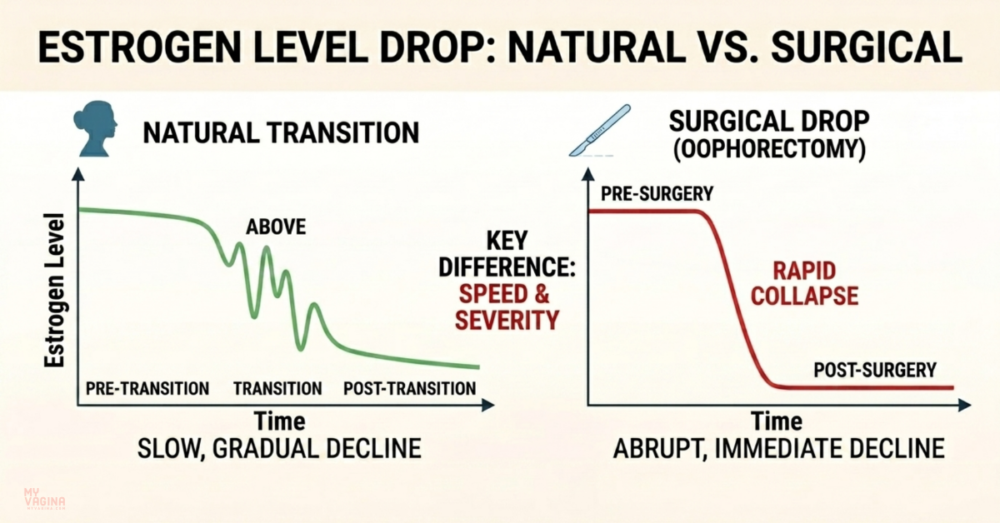
The difference comes down to speed. In natural menopause, oestrogen and other ovarian hormones decline gradually over several years, so the tissues of the vulva, vagina, urethra and bladder have time to adjust.2
When both ovaries are removed, that supply is switched off almost overnight. The abrupt loss of oestrogen and androgens produces a sharper drop than the body has ever had to cope with, which can mean more intense vasomotor symptoms, mood changes and sexual difficulties.3
That same abrupt loss is what drives a more severe GSM phenotype. The genitourinary tissues are densely studded with oestrogen receptors, so when oestrogen disappears suddenly, the lining thins, loses elasticity and produces less natural moisture faster than it would in a slow, natural transition.2,4
GSM is more than dryness
GSM is the modern umbrella term, agreed in 2014, for what used to be called vulvovaginal atrophy or atrophic vaginitis. It was renamed precisely because atrophy undersold how much it affects.5 You can read more in our explainer on how atrophic vaginitis got a new name.
The syndrome covers three overlapping groups of symptoms:
- Genital: dryness, burning, itching and irritation of the vulva and vagina
- Sexual: poor lubrication, discomfort or pain with sex (dyspareunia) and reduced desire
- Urinary: urgency, frequency, painful urination and recurrent urinary tract infections (UTIs)
GSM affects somewhere between 27 and 84 per cent of postmenopausal women, depending on how it is measured.4 Unlike hot flushes, which often fade with time, GSM tends to be progressive and does not resolve on its own without treatment.2
What this means for you
If you have had both ovaries removed, whether for cancer risk, endometriosis, or alongside a hysterectomy, this is your cue to take genitourinary symptoms seriously and early, rather than waiting until things are uncomfortable.
In our experience here at My Vagina, the urinary side of GSM is the part that gets missed most often. Recurrent UTIs, urgency and burning on weeing are frequently blamed on infection alone, when low oestrogen in the bladder and urethra is quietly driving the problem. We see it in people years after surgery.
It is also worth knowing that low-oestrogen tissue can be misread on a swab. A microbiome result that looks like an infection can sometimes be atrophy instead. This is a trap we have written about in our practitioner case on a post-hysterectomy BV result that turned out to be atrophy.
None of this is a reason to panic. It is a reason to be proactive. GSM is manageable, and catching it early gives the tissues the best chance.
FAQ
What is surgical menopause?
Surgical menopause is menopause triggered by removing both ovaries (bilateral oophorectomy), often at the same time as a hysterectomy. Because the ovaries are the main source of oestrogen before menopause, removing them causes an immediate and steep hormone drop rather than a gradual decline.
Is GSM worse after surgical menopause than natural menopause?
The new study suggests yes. Women with surgical menopause reported more urinary symptoms, more painful sex and lower sexual desire than women in natural menopause.1 The sudden hormone loss is thought to be the reason.
Will GSM go away by itself?
No. Unlike hot flushes, GSM tends to be ongoing and progressive without treatment, because the underlying cause, low oestrogen in the genitourinary tissues, does not correct itself.2
Can GSM be treated?
Yes. There are well-established options, and the right approach depends on your history and symptoms. This is a conversation to have with a clinician who understands menopause and genitourinary health.
What to do next
If you have been through surgical menopause and have any vaginal, sexual or urinary symptoms, do not wait them out. Talk to a clinician who knows GSM, and ask specifically about the urinary side, not just dryness.
If your symptoms come with an unusual discharge or an odd swab result, a thorough PCR or NGS microbiome test can help tell genuine infection apart from low-oestrogen changes that only look like infection.
You can also ask Aunt Vadge’s Assistant, the chat widget in the bottom left of the screen, to point you towards the right information, or book in with one of our practitioners.
This is general information, not a substitute for personalised medical advice. If you have symptoms, please see a qualified clinician.
- Ozmen S, et al. Study on the genitourinary syndrome of menopause phenotype in surgical versus natural menopause. Menopause. 2026 (advance online publication). Reported in: Surgical Menopause Tied To Worse Sexual And Urinary Symptoms.
- Faubion SS, Sood R, Kapoor E. Genitourinary Syndrome of Menopause: Management Strategies for the Clinician. Mayo Clin Proc. 2017;92(12):1842–1849.
- Faubion SS, Kuhle CL, Shuster LT, Rocca WA. Long-term health consequences of premature or early menopause and considerations for management. Climacteric. 2015;18(4):483–491.
- Nguyen H. Genitourinary Syndrome of Menopause. In: StatPearls. StatPearls Publishing; 2024.
- Portman DJ, Gass MLS. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Menopause. 2014;21(10):1063–1068.


