
Uterine hypoplasia means the uterus is smaller than it should be, having failed to grow to its full adult size. It is a congenital anatomical difference – the uterus is built that way before birth or simply never catches up during puberty – and it is most often discovered when a young person doesn’t start their periods, or later when they have trouble conceiving.1
It sits on a spectrum. At one end the uterus is just on the small side; at the other it has stayed the size and shape of a child’s, a pattern doctors call an infantile uterus.1 A hypoplastic uterus can appear on its own, or alongside other differences in the cervix, vagina or ovaries.1
In our clinic, a small uterus is rarely the headline – it’s usually a clue pointing upstream to the hormonal or developmental story behind it, and that’s where we put our attention.
What is uterine hypoplasia (a small uterus)?
The word hypoplasia comes from the Greek for ‘under’ and ‘formation’, so a hypoplastic uterus is simply one that hasn’t reached full development.1 In practical terms, clinicians describe a uterus as hypoplastic when its total length, measured from the external opening of the cervix to the top of the uterus, is under about 6cm.1
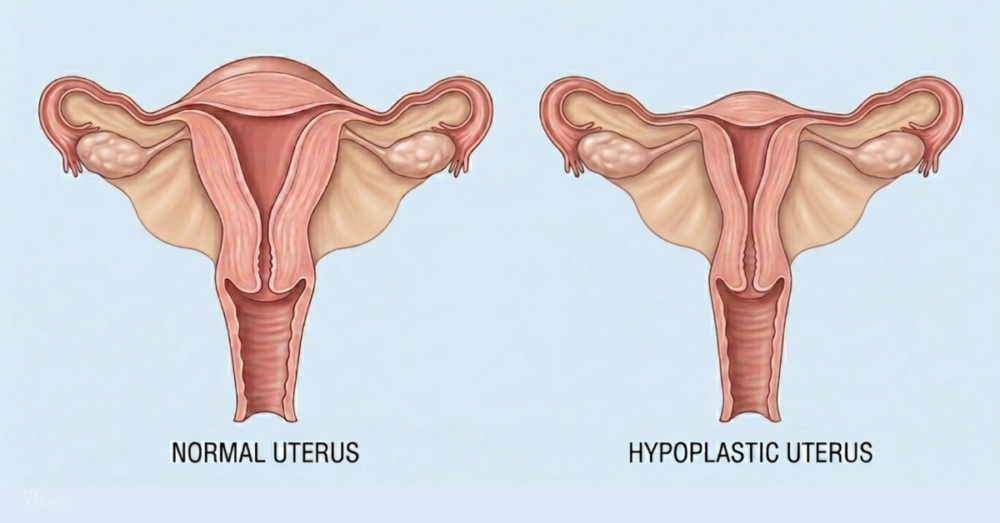
A normally developed adult uterus is roughly pear-shaped and about 7 to 8cm long, with the muscular body making up about two-thirds of its length and the cervix about one-third – a body-to-cervix ratio of around 2:1.1 Before puberty, that ratio is reversed: a child’s uterus is mostly cervix.1 The surge of hormones at puberty is what grows the body of the uterus into its adult proportions, and uterine hypoplasia is, at heart, a story of that growth not happening fully.1
Hypoplastic uterus or infantile uterus, what’s the difference?
These two terms get used loosely, and even in the medical literature there is no single agreed definition.1–2 The most useful way to separate them is by that body-to-cervix ratio.
- A hypoplastic uterus keeps the normal adult 2:1 ratio – it is built in the right proportions, just smaller all over.1
- An infantile uterus has kept the childhood proportions, with a ratio of about 1:1 or even 1:2, so the cervix makes up half or more of its length.1
The distinction matters because it hints at what went wrong and when. An infantile uterus suggests development stalled before puberty got going, whereas a proportionate but small uterus suggests growth was simply blunted along the way.1–2 Some specialists argue the two should be clearly separated in classification systems rather than lumped together, precisely because the underlying problem differs.2
What causes uterine hypoplasia?
Honest answer: in most individual cases the exact cause is never pinned down.1 What is generally accepted is that the common thread is a shortfall in the hormonal signals that should drive uterine growth – most often a lack of oestrogen, or a problem somewhere along the hormonal chain from the brain to the ovaries.1 That’s why a small uterus so often travels with delayed puberty and absent periods.
Several recognised conditions can produce a small or underdeveloped uterus:
- MRKH syndrome (Mayer-Rokitansky-Küster-Hauser), in which the uterus and upper vagina are absent or underdeveloped despite normal ovaries and breast development – one of the most common causes of an absent period from birth.1
- Turner syndrome, where part or all of an X chromosome is missing; a small uterus is common, particularly with the 45,X pattern.1
- Swyer syndrome and other differences of sexual development, where the gonads don’t produce the hormones needed to mature the uterus.1
- Hyperprolactinaemia arising before puberty is complete, which can suppress the hormonal signals that grow the uterus.1
- Pituitary, thyroid or ovarian under-function, and rarer genetic conditions such as Perrault syndrome or a fault in the follicle-stimulating hormone receptor.1
- In-utero exposure to diethylstilboestrol (DES), a synthetic oestrogen prescribed to pregnant women until the 1970s, which is a well-documented cause of a small, tube-shaped uterus in the daughters who were exposed.1
Severe chronic illness, significant undernutrition and eating disorders in the growing years have also been linked to delayed uterine development, because the body deprioritises reproduction when it is under strain.1 This is the kind of upstream picture worth taking seriously rather than treating the uterus in isolation.
Symptoms and signs
The external genitals usually look completely typical, so there is rarely anything visible to give it away.1 Instead, uterine hypoplasia tends to announce itself through what isn’t happening.
- Periods that never start (primary amenorrhoea), or very light, scanty periods.1
- Painful, cramping periods, thought to relate to the unusual muscle-to-tissue make-up of a small uterus.1
- Difficulty conceiving, or repeated pregnancy loss.1
- Pain or tightness with sex, especially where the vagina is also short or underdeveloped.1
Because the ovaries are often working normally, many people with a hypoplastic uterus do develop breasts and pubic hair on schedule – the absent period is what eventually prompts a closer look.1
How uterine hypoplasia is diagnosed
Diagnosis usually starts when a teenager hasn’t menstruated by the expected age, or when an adult is being investigated for infertility or recurrent miscarriage.1 The work-up is methodical, and the point is as much to find the cause as to confirm the small uterus.
Typical steps include a pelvic examination, blood tests to map the hormones (and sometimes a chromosome test), and imaging.1,3 Ultrasound is the usual first imaging step and can measure the uterus directly; a total length under about 6cm, a short cervix or a narrowed cavity all point towards hypoplasia.1,3 Magnetic resonance imaging (MRI) gives a more detailed map of the uterus, cervix, vagina and surrounding structures, which matters because differences rarely come one at a time.3
Two further tools may be used to look inside the cavity itself. Hysterosalpingography (an X-ray with dye) can show a small, tube-shaped or T- or Y-shaped cavity, while hysteroscopy – a thin camera passed through the cervix – lets a specialist see the cavity directly and, in the same sitting, sometimes treat it.1,3 In our experience, the calm, thorough version of this work-up is worth holding out for, because a one-line diagnosis with no context leaves people far more frightened than the situation usually warrants.
Where it fits in the classification systems
Congenital differences of the uterus, cervix and vagina are grouped under what doctors call müllerian anomalies, after the embryonic ducts that form these organs. They are not rare, affecting somewhere in the order of 4 to 7 per cent of people with a uterus.4
Two main systems are used to classify them. The American Society for Reproductive Medicine (ASRM) updated its system in 2021, sorting anomalies into clear descriptive categories based on imaging.5 The European system from ESHRE and ESGE is the only one of the two that names the infantile uterus specifically, filing it under a sub-category for a normal-shaped but underdeveloped uterus with the childhood body-to-cervix proportions.4
This is an area of genuine debate – specialists don’t fully agree on where a hypoplastic or infantile uterus belongs, or even on the exact measurements that define them.2 For you, the practical takeaway is that a precise, well-described diagnosis matters more than the label, because it guides what comes next.2
Fertility and pregnancy
This is usually the question people most want answered, and the honest version is that it depends heavily on the degree of underdevelopment and on what is causing it.1 A mildly small but otherwise normal uterus with working ovaries has a very different outlook from an infantile uterus tied to a chromosomal or hormonal condition.
Difficulty conceiving and a higher risk of miscarriage and preterm birth are well described, partly because the cavity is small and the endometrial lining (where an embryo implants) is often thin, and partly because of the hormonal conditions that caused the hypoplasia in the first place.1 Reported pregnancy outcomes in the older case series are sobering, though these studies are small and many involved DES-exposed uteri, so they don’t necessarily reflect what’s possible today.1
Where the ovaries are functioning, eggs can often be retrieved, which keeps options open – including, in some situations, assisted reproduction or a surrogate or gestational carrier.1 For people whose uterus cannot carry a pregnancy, uterus transplantation has moved from experimental to occasionally available in specialist centres, although it remains a major undertaking. None of this is a decision to make alone or quickly, and a reproductive specialist is the right person to map out realistic options for a specific situation.
Treatment options
There is no quick fix, and it’s worth saying plainly that the evidence for every treatment here is limited.1 Management follows the cause, which is exactly why the diagnostic work-up matters so much.
Hormonal therapy
Because oestrogen drives uterine growth at puberty, oestrogen therapy is a long-standing approach, and it works best where the problem is a clear oestrogen deficiency in someone whose uterus can still respond.1 Some people see real growth in the uterus on hormonal treatment; in others the gain is small or temporary.1 Where hypoplasia is part of a wider condition such as ovarian or pituitary failure, hormone replacement also protects bones and general health, well beyond the uterus itself.
Surgical approaches
For selected people with a small cavity and a history of infertility or miscarriage, a hysteroscopic procedure to gently enlarge the uterine cavity has been described, usually followed by a short course of hormones.1 Reported pregnancy rates after this kind of surgery are encouraging in small series, but the numbers are small and it is not a routine offering.1 Any surgery here belongs firmly in the hands of a specialist in congenital uterine differences.
Treating the cause, not just the measurement
The thread running through all of this is that the uterus is the part that gets measured, but the answer usually lives upstream – in the endocrine system, the chromosomes, or the developmental history. In our experience, supporting the whole person, and correcting what’s driving the underdevelopment where that’s possible, is more useful than fixating on a single number on a scan.
Living with a uterine difference
A diagnosis like this can land hard, especially when it arrives in your teens or right when you’re hoping to start a family. The word ‘malformed’ does a lot of unnecessary damage – your body is not broken, it has simply developed along a different path, and you are not alone in it.
A hypoplastic uterus rarely travels by itself, so it’s worth understanding the related differences too, such as cervical hypoplasia, vaginal agenesis and other müllerian duct anomalies. Good care here is rarely just medical – psychological support, and where wanted, peer connection with others who have the same diagnosis, makes a real difference.
Frequently asked questions
Can you get pregnant with a small uterus?
Sometimes, yes – it depends on how underdeveloped the uterus is and what caused it. A mildly small uterus with healthy ovaries has a far better outlook than a severely infantile one. Conceiving may be harder and pregnancy higher-risk, so specialist reproductive care is important.1
Is uterine hypoplasia the same as not having a uterus?
No. Hypoplasia means the uterus is present but small or underdeveloped. A completely absent uterus is a separate finding, seen for example in some cases of MRKH syndrome, although MRKH can also produce a small underdeveloped uterus rather than none at all.1
How is it diagnosed?
Through a combination of hormone blood tests and imaging. Ultrasound measures the uterus, and an MRI gives a fuller picture of the uterus, cervix and vagina. Hysteroscopy may be used to look inside the cavity directly.1,3
What size uterus counts as hypoplastic?
There’s no universally agreed cut-off, but a total uterine length under about 6cm is the most commonly used threshold, alongside the body-to-cervix ratio that separates a hypoplastic uterus from an infantile one.1–2
What is the normal size of a uterus?
A fully developed adult uterus is roughly 7.5 to 8cm long, with the muscular body making up about two-thirds and the cervix about one-third. A uterus under about 6cm long is generally considered small or hypoplastic, though the proportions matter just as much as the length.1
Will hormone treatment make my uterus grow?
It can, particularly where the cause is an oestrogen deficiency and the uterus is still able to respond. Results vary a lot between people, and some growth can be temporary, so it’s something to discuss with a specialist.1
Is uterine hypoplasia common?
Congenital uterine differences as a group affect roughly 4 to 7 per cent of people with a uterus, but hypoplasia specifically is much less common, and good prevalence figures are hard to come by because definitions vary.2,4
What to do next
If you or your teenager hasn’t started periods by around 15, or you’re facing unexplained infertility or repeated miscarriage, this is worth raising with a gynaecologist or reproductive specialist. Ask for proper imaging and a hormonal work-up so you understand the whole picture, not just the headline.
If you’d like to talk something through, Aunt Vadge’s Assistant is in the bottom-left of your screen, and our practitioners are here if you want a closer look at your specific situation. You don’t have to make sense of a diagnosis like this on your own.
This article is general information, not a substitute for personalised medical advice. If uterine hypoplasia is suspected, please see a gynaecologist or reproductive specialist.
- Alonso Pacheco L, Carugno J, Alcázar JL, et al. Infantile uterus and uterine hypoplasia: a comprehensive overview to explore possible managements amidst limited scientific certainties. Facts Views and Vision in ObGyn. 2025;17(1):5–14.
- Küçük T, Ata B. Infantile or hypoplastic uterus? A proposal for a modification to the ESHRE/ESGE classification of female genital tract congenital abnormalities. Facts, Views and Vision in ObGyn. 2022;14(1):49–50.
- Passos IMPE, Britto RL. Diagnosis and treatment of müllerian malformations. Taiwan J Obstet Gynecol. 2020;59(2):183–188.
- Grimbizis GF, Gordts S, Di Spiezio Sardo A, et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum Reprod. 2013;28(8):2032–2044.
- Pfeifer SM, et al. ASRM müllerian anomalies classification 2021. Fertil Steril. 2021;116(5):1238–1252.


